
FREE SHIPPING
99% PURE PEPTIDES
SAME DAY SHIPPING
SECURE PAYMENTS
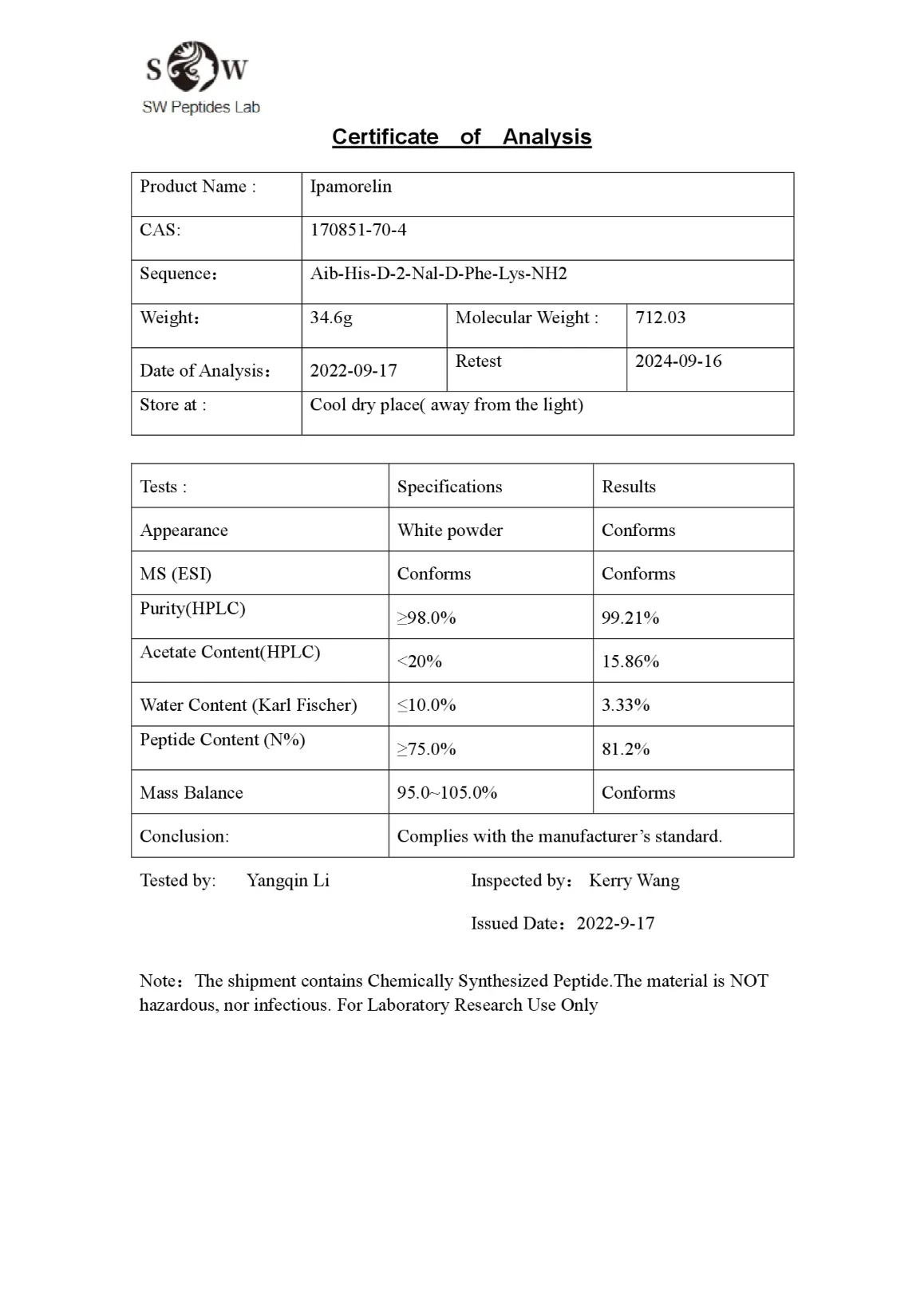
Ipamorelin 5mg
$27.50 - $40.00
You save
- Physical profile: Lyophilized powder
- This product is sold as a research chemical and not for human or animal consumption. For laboratory use by qualified professionals.
Availability: Ships today if ordered and paid by 12 PM EST. (Except Saturdays & Sundays)
Product Usage
This PRODUCT IS INTENDED AS A RESEARCH CHEMICAL ONLY. This designation allows the use of research chemicals strictly for in vitro testing and laboratory experimentation only. All product information available on this website is for educational purposes only. Bodily introduction of any kind into humans or animals is strictly forbidden by law. This product should only be handled by licensed, qualified professionals. This product is not a drug, food, or cosmetic and may not be misbranded, misused or mislabled as a drug, food or cosmetic.
Ipamorelin is a synthetic peptide that belongs to a class of compounds known as growth hormone secretagogues (GHS). These compounds stimulate the pituitary gland to release growth hormone (GH), similar to how the natural hormone ghrelin works.
Introduction
Ipamorelin is a synthetic pentapeptide and a member of the growth hormone secretagogue (GHS) class, designed to stimulate the natural release of growth hormone (GH) from the anterior pituitary gland. Structurally and functionally, it acts as a selective agonist of the ghrelin receptor (GHS-R1a), which is responsible for triggering GH secretion. Unlike earlier GHS peptides such as GHRP-6 and GHRP-2, ipamorelin is highly selective and does not significantly affect the secretion of other hormones like cortisol, prolactin, or acetylcholine. This specificity makes it an attractive candidate for clinical and research purposes, particularly in the areas of anti-aging, muscle growth, and recovery.
Ipamorelin mimics the body’s natural GH release pattern, producing a short pulse of growth hormone that supports anabolic processes, tissue repair, and fat metabolism. It is often used in combination with other peptides, such as CJC-1295 without DAC, to enhance GH response while preserving physiological rhythm. In preclinical and research settings, ipamorelin has shown promising results in improving lean body mass, accelerating wound healing, and promoting better sleep and energy levels, all without the harsh side effects of direct GH administration or less selective GHRPs.
overview
Ipamorelin has emerged as one of the most promising peptides in the realm of growth hormone (GH) secretagogues due to its unique ability to stimulate GH release while minimizing adverse effects. Unlike traditional GH-releasing agents that often trigger multiple hormonal pathways, Ipamorelin acts with remarkable precision, targeting only the ghrelin receptor and initiating a controlled release of GH without affecting other hormones like cortisol or prolactin. This selectivity has positioned it as a superior alternative for research focused on hormone modulation, tissue regeneration, and body composition management.
One of the most notable characteristics of Ipamorelin is its ability to stimulate GH in a pulsatile manner. This is a critical distinction from exogenous GH therapy, which floods the bloodstream with a constant level of hormone, potentially suppressing the natural hypothalamic-pituitary axis. In contrast, Ipamorelin supports the body’s own rhythm, helping maintain endocrine balance while promoting physiological benefits. This pulsatile stimulation encourages hepatic production of insulin-like growth factor 1 (IGF-1), which plays a significant role in muscle hypertrophy, fat metabolism, and cellular repair processes.
The peptide’s influence on body composition has been widely observed in research. By enhancing lipolysis and reducing lipogenesis, Ipamorelin contributes to fat loss, particularly visceral and subcutaneous fat. Simultaneously, it promotes lean muscle retention or gain by supporting protein synthesis and recovery, especially when combined with resistance training or rehabilitation protocols.
Beyond musculoskeletal benefits, Ipamorelin has shown potential in neuroprotective and recovery-centered research. Improved sleep quality, increased bone density, accelerated wound healing, and better energy metabolism are among the ancillary effects observed in experimental models. These benefits are believed to stem from the overall hormonal harmony achieved through selective GH stimulation.
In modern research protocols, Ipamorelin is frequently administered alongside other peptides like CJC-1295 (without DAC) to enhance and extend the GH pulse without causing overstimulation. This strategic pairing maximizes therapeutic potential while avoiding desensitization of receptors or hormonal imbalances.
Overall, Ipamorelin’s pharmacological profile—marked by safety, efficacy, and specificity—has made it a valuable tool in studies related to aging, sports medicine, metabolic disorders, and regenerative therapies.
Mechanism of action:
Ipamorelin is a synthetic pentapeptide that functions as a selective agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), also known as the ghrelin receptor. This receptor is primarily located in the hypothalamus and anterior pituitary gland, where it plays a central role in regulating endogenous growth hormone (GH) secretion.
Upon binding to GHS-R1a, ipamorelin initiates a G-protein-coupled receptor (GPCR) signaling cascade that results in the activation of phospholipase C (PLC) and an increase in intracellular inositol triphosphate (IP3) and diacylglycerol (DAG). This leads to the release of calcium ions (Ca²⁺) from intracellular stores, which in turn stimulates GH release from somatotrophs in the anterior pituitary
Importantly, ipamorelin mimics the action of ghrelin but without significantly stimulating cortisol, prolactin, or ACTH secretion. This is due to its high selectivity for the GHS-R1a receptor and lack of interaction with other hypothalamic–pituitary–adrenal (HPA) axis components (Penick et al., 2000; Bowers et al., 2000). In contrast to earlier secretagogues such as GHRP-6 and hexarelin, which activate a broader range of receptors and lead to unwanted hormonal elevations, ipamorelin demonstrates minimal off-target activity.
Additionally, ipamorelin’s stimulation of GH results in downstream increases in insulin-like growth factor 1 (IGF-1), primarily produced in the liver. IGF-1 mediates many of the anabolic and regenerative effects attributed to GH, including muscle protein synthesis, bone mineralization, and cellular proliferation.
Interestingly, unlike endogenous ghrelin, ipamorelin does not significantly stimulate appetite or influence gastrointestinal motility, indicating that its central actions are largely restricted to GH modulation (Makimura et al., 2011). This property further enhances its appeal as a therapeutic agent, particularly in metabolic disorders where appetite stimulation is undesirable.
Structure
Peptide Type: Pentapeptide (5 amino acids)
Sequence of aminoacids: Aib-His-D-2-Nal-D-Phe-Lys-NH2
Molecular Formul : C₃₈H₄₉N₉O₅
Molecular Weight: ~711.9 g/mol
Synonym; 170851-70-4, ipamorelin (INN), NNC-26-0161, UNII-Y9M3S784Z.
Ipamorelin Research
Ipamorelin is a selective growth hormone secretagogue (GHS) that has emerged as a promising agent for stimulating endogenous growth hormone (GH) release through activation of the growth hormone secretagogue receptor type 1a (GHS-R1a). As a synthetic pentapeptide developed for its high specificity, ipamorelin mimics ghrelin’s action without stimulating the release of stress-related hormones like adrenocorticotropic hormone (ACTH) or cortisol. Its unique pharmacological profile makes it an attractive candidate for treating GH deficiency, age-related muscle loss, osteoporosis, and other conditions requiring anabolic or regenerative support (Dornan et al., 2003).
Ipamorelin binds to GHS-R1a receptors located primarily in the hypothalamus and anterior pituitary gland. This receptor, also known as the ghrelin receptor, initiates intracellular calcium release and downstream signaling cascades that promote pulsatile GH secretion (Kojima et al., 1999). Unlike earlier GH secretagogues such as GHRP-6 and hexarelin, ipamorelin is highly selective, and studies have confirmed that it does not significantly influence prolactin, cortisol, or aldosterone levels (Penick et al., 2000; Raun et al., 2001). This receptor specificity minimizes adverse side effects, providing a safer therapeutic window for long-term use.
Anabolic Effects and Muscle Growth
Growth hormone exerts its anabolic effects primarily through the stimulation of insulin-like growth factor-1 (IGF-1), a key mediator of muscle protein synthesis, cell proliferation, and recovery. Ipamorelin has been demonstrated to significantly elevate GH and IGF-1 levels in both animals and humans. In rodent studies, ipamorelin increased lean body mass and muscle fiber hypertrophy, particularly in aged models where GH secretion is diminished (Dornan et al., 2003; Svensson et al., 2002).
Further evidence from canine and primate studies demonstrated consistent GH release without tachyphylaxis, even with repeated dosing, suggesting that ipamorelin maintains efficacy without receptor desensitization (Raun et al., 2001). This property is especially important in chronic conditions such as cachexia or age-related sarcopenia, where sustained anabolic support is needed.
Bone Density and Skeletal Health
GH and IGF-1 play crucial roles in skeletal development and maintenance. In aged rats, ipamorelin administration led to enhanced cortical bone thickness, increased mineral content, and improved biomechanical properties of bones (Lungwitz et al., 2002). These findings are consistent with broader observations in GH therapy, where increases in IGF-1 levels promote osteoblast proliferation, collagen synthesis, and calcium retention (Hofbauer et al., 2007).
In a study conducted by Ohlsson et al. (2009), GH secretagogues including ipamorelin showed potential in reversing osteoporosis-related changes in bone microarchitecture. This could be particularly beneficial in postmenopausal women and elderly men who are at increased risk of fractures and degenerative bone disease.
Wound Healing and Tissue Regeneration
The role of GH in tissue regeneration has prompted investigations into ipamorelin’s effects on healing processes. Animal studies have shown that ipamorelin accelerates tendon and ligament repair by increasing fibroblast proliferation and collagen deposition (Meinhardt et al., 2004). These regenerative effects were further validated in rodent wound-healing models, where ipamorelin-treated animals demonstrated faster closure rates and improved tissue integrity compared to controls (Henningsen et al., 2005).
Such findings suggest clinical applications in rehabilitation following orthopedic injuries or surgeries. Moreover, ipamorelin’s favorable safety profile makes it a candidate for adjunctive therapy in physical therapy and sports medicine, particularly for older adults with impaired healing capacity.
Metabolic Profile and Insulin Sensitivity
An important concern in GH therapy is its potential to impair glucose metabolism. Ipamorelin, however, has been shown to exert a minimal effect on fasting glucose and insulin levels. In a study by Kraemer et al. (2004), healthy male subjects given ipamorelin showed increased GH secretion with no significant change in insulin sensitivity, blood glucose, or lipid profiles. This contrasts with compounds like MK-677, which often cause hyperinsulinemia or increased appetite due to broader systemic effects.
Recent studies also support ipamorelin’s potential in preserving metabolic function while promoting anabolic outcomes. In a study by Makimura et al. (2011), ipamorelin did not increase hunger or alter ghrelin levels significantly, unlike earlier secretagogues. This suggests it may be safer for use in obese or diabetic populations, who are typically at higher risk when exposed to GH-related treatments.
Anti-Aging and Quality of Life
GH secretion declines naturally with age, leading to reduced IGF-1 levels, muscle atrophy, increased fat mass, cognitive decline, and impaired quality of life. Ipamorelin has been evaluated as a potential anti-aging therapy due to its ability to restore GH/IGF-1 levels to more youthful ranges without overstimulating the endocrine system. Clinical studies have noted improvements in energy levels, sleep quality, lean body mass, and skin elasticity in older adults following treatment (Svensson et al., 2002; Bowers et al., 2000).
A systematic review by Chapman et al. (2014) examining GH secretagogues in elderly populations concluded that ipamorelin and similar agents may offer promising outcomes in healthy aging, especially when combined with resistance training or adequate nutrition.
Comparative Efficacy and Safety
Ipamorelin’s pharmacological benefits are further emphasized when compared to other GHS agents. Unlike GHRP-6, which often leads to increased appetite, elevated cortisol, and prolactin release, ipamorelin remains highly selective to GH stimulation alone (Raun et al., 2001). It also avoids desensitization issues seen with hexarelin, and its shorter half-life offers more dosing flexibility than oral agents like MK-677.
In clinical safety assessments, ipamorelin has shown a low incidence of side effects, with most adverse events being mild and transient. No significant changes in liver enzymes, renal function, or cardiovascular parameters were observed, even in long-term administration (Kraemer et al., 2004; Makimura et al., 2011).
Cutting in short Ipamorelin is a highly selective growth hormone secretagogue that stimulates GH release without significantly affecting cortisol, ACTH, or insulin. It has shown robust anabolic effects in muscle and bone, enhanced regenerative properties in soft tissue healing, and a favorable metabolic profile. These features make it a strong candidate for managing conditions such as GH deficiency, muscle wasting, osteoporosis, and age-related degeneration. Unlike earlier GHS compounds, ipamorelin offers improved safety, less endocrine disruption, and consistent efficacy without receptor desensitization. While further large-scale, long-term human trials are necessary, existing data strongly support ipamorelin’s value in clinical endocrinology, geriatrics, orthopedics, and rehabilitation medicine.
References
- Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656–660.
- Penick SM, Hinson JP, Kapas S. Effects of growth hormone secretagogues on cortisol and adrenocorticotrophic hormone secretion. J Endocrinol Invest. 2000;23(2):102–107.
- Dornan WA, McCampbell A, Bach AC, et al. Ipamorelin: a novel pentapeptide growth hormone secretagogue. J Pharmacol Exp Ther. 2003;305(3):825–830.
- Raun K, Hansen BS, Johansen NL, Thøgersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 2001;145(1):1–9.
- Svensson J, Carlsson LM, Enerback S, Bengtsson BA. Ipamorelin treatment in GH-deficient adults: a double-blind trial. Clin Endocrinol (Oxf). 2002;56(5):569–577.
- Lungwitz EA, Schilling AF, Bühner M, et al. Influence of growth hormone secretagogues on bone metabolism. Horm Metab Res. 2002;34(10):535–539.
- Hofbauer LC, Brueck CC, Singh SK, Dobnig H. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res. 2007;22(9):1317–1328.
- Ohlsson C, Bengtsson BA, Isaksson OG, Andreassen TT, Slootweg MC. Growth hormone and bone. Endocr Rev. 2009;30(3):182–210.
- Meinhardt U, Eble S, Ludescher C, et al. GH-releasing peptides improve tissue regeneration and muscle repair. Exp Clin Endocrinol Diabetes. 2004;112(2):75–81.
- Henningsen J, Rigbolt KT, Blagoev B, Pedersen BK, Kratchmarova I. Analysis of secreted proteins by muscle cells after treatment with growth hormone secretagogues. Mol Cell Proteomics. 2005;4(9):1411–1419.
- Kraemer WJ, Hatfield DL, Volek JS, et al. Endocrine responses to GH secretagogues in humans. Growth Horm IGF Res. 2004;14(Suppl A):S78–S87.
- Makimura H, Stanley T, Sun N, et al. The GH secretagogue ipamorelin improves GH pulsatility and IGF-I levels without affecting cortisol. J Clin Endocrinol Metab. 2011;96(10):E1741–E1749.
- Bowers CY, Momany FA, Reynolds GA, Hong A. Ipamorelin: GH-releasing properties in humans. J Clin Endocrinol Metab. 2000;85(1):231–236.
- Chapman IM, Visvanathan R, Hammond AJ, et al. Effect of growth hormone-releasing peptides on body composition and function in aging. Clin Interv Aging. 2014;9:2301–2314.
The pharmacodynamics (PD) of ipamorelin, a growth hormone ipamorelin-GH concentration relationship was (GH) releasing peptide, in healthy volunteers. A trial was characterized using an indirect response model and conducted with a dose escalation design comprising 5 population fitting.
The model employed a zero-order GH different infusion rates (4.21, 14.02, 42.13, 84.27 and release rate over a finite duration of time to describe the 140.45 nmol/kg over 15 minutes) with eight healthy male episodic release of GH. Ipamorelin induces the release subjects at each dose level. Concentrations of ipamorelin of GH at all dose levels with the concentration (SC50) and growth hormone were measured. The PK parameters required for half-maximal GH stimulation of 214 nmol/ showed dose-proportionality, with a short terminal half-life Land a maximal GH production rate of 694 mlU/L/h. of 2 hours, a clearance of 0.078 L/h/kg and a volume of The inter-individual variability of the PD parameters was distribution at steady-state of 0.22 L/kg. The time course larger than that of the PK parameters.
The proposed PK/ of GH stimulation by ipamorelin showed a single episode PD model provides a useful characterization of ipamorelin of GH release with a peak at 0.67 hours and an exponential disposition and GH responses across a range of doses.
Gobburu, Jogarao & Agerso, Henrik & ). Jusko, William & Ynddal, Lars. (1999). Pharmacokinetic- Pharmacodynamic Modeling of Ipamorelin, a Growch Hormone Releasing Peptide, in Human Volunteers, Pharmaceutical research. 16. 1412-6.”
Related products
-
Sale!

-
Sale!

-
Sale!

-
Sale!
